Self-cycleTM IVF
Self-cycleTM IVF

-
-
-
 Infertility Counselling
Infertility Counselling
-
 Female Infertility Treatment
Female Infertility Treatment
-
 Andrology Treatment
Andrology Treatment
-
 Fertility Enhancing Surgeries - Female
Fertility Enhancing Surgeries - Female
-
 Fertility Enhancing Surgeries - Male
Fertility Enhancing Surgeries - Male
-
 Endoscopy Treatment
Endoscopy Treatment
-
 IUI Treatment
IUI Treatment
-
 IVF Treatment
IVF Treatment
-
 ICSI Treatment
ICSI Treatment
-
 Advance IVF Solutions
Advance IVF Solutions
-
 Embryology
Embryology
-
 Vitrification Egg, Embryo, Sperm Freezing
Vitrification Egg, Embryo, Sperm Freezing
-
 Preimplantation Genetic Testing (PGT)
Preimplantation Genetic Testing (PGT)
-
 Donation Program Embryo / Egg / Sperm
Donation Program Embryo / Egg / Sperm
-
 Self-cycleTM IVF
Self-cycleTM IVF
-
-
-
-
-
Fresh vs Frozen Embryo Transfer: What the Science Says and Which Option Suits You Best

When patients have reached the point where embryo transfer is necessary, they have already undergone weeks of medications, testing, injections, and the roller coaster that goes along with IVF.
Being told whether a fresh vs frozen embryo transfer is preferable can add another layer of confusion, especially when it feels like a decision that directly affects the outcome. The good news is that this choice is guided by clear clinical reasoning.
What Is a Fresh Embryo Transfer?
In a fresh embryo transfer, the embryo created during the egg retrieval cycle is transferred directly into the uterus 3 to 5 days later, within the same IVF cycle. It does not involve freezing of the embryos.
The retrieval and the transfer happen in sequence, making this the more immediate of the two approaches.
What Is a Frozen Embryo Transfer (FET)?
In a frozen embryo transfer, also known as FET, embryos are first cultured in the IVF lab for a few days after fertilisation. The embryology team decided whether to freeze them at the cleavage stage on Day 3 or at the blastocyst stage on Day 5 or Day 6. These frozen embryos are then thawed and transferred in a later cycle, when the uterus is better prepared for implantation.
The freezing method used today is commonly called vitrification, which helps maintain very high embryo survival rates after thawing.
Among the different types of embryo transfer in IVF, FET is often recommended when a freeze-all approach is needed. This may be advised in certain cases such as risk of ovarian hyperstimulation syndrome (OHSS), endometrial synchronisation issues, uterine concerns, or when genetic testing such as PGT is planned before embryo transfer.

Fresh vs Frozen Embryo Transfer: Key Differences at a Glance
The two approaches differ not only in timing but in the biological environment they create for implantation. For patients weighing fresh embryo transfer vs frozen embryo transfer, the clinical differences between the two ultimately guide the decision.
Timing and Cycle Structure
The fresh embryo transfer involves the placement of the embryo into the womb shortly after the egg retrieval procedure, with everything being done in the same IVF cycle.
Whereas frozen embryo transfer is a process which requires a bit more time since it involves the preservation of the embryo first, and then the actual implantation after several weeks, allowing more recovery time.
Uterine Receptivity and Hormonal Environment
High hormone levels after ovarian stimulation can sometimes affect implantation conditions in a fresh cycle. Frozen embryo transfer creates separation between retrieval and transfer, allowing the uterine lining to develop in a more controlled and stable environment.
Ovarian Hyperstimulation Syndrome (OHSS) Risk
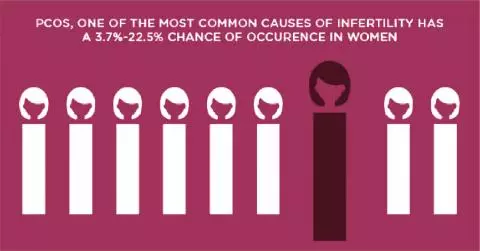
In the case of patients with PCOS or a high ovarian response, going for a fresh transfer increases the chances that their OHSS symptoms become worse.
A frozen embryo transfer is deemed a safer option since the body gets time to recuperate before implantation.
Suitability for Preimplantation Genetic Testing (PGT)
PGT embryos require a period of time for biopsy and analysis prior to being transferred, which makes the transfer of frozen embryos the preferred method.
Since the embryos need to be preserved while test results are being reviewed, effective freezing and thawing techniques play an important role in maintaining embryo quality. At Nova IVF Fertility, advanced embryology practices support this process and help ensure embryos remain viable for transfer.
Is Frozen Embryo Transfer Better Than Fresh Embryo Transfer? What the Research Shows
Research does not suggest that one transfer type is automatically better for everyone. When it comes to fresh vs frozen IVF transfer, success rates often depend on hormone levels, ovarian response, PCOS status, and overall treatment planning.
| Patient Situation | What Research Commonly Shows |
|---|---|
| Women with PCOS or high ovarian response | Frozen embryo transfer often shows equal or higher live birth rates because the body gets recovery time after stimulation |
| Patients planning PGT or genetic testing | Frozen transfer is usually preferred because embryos need time for testing before implantation |
| Younger women with stable hormone levels | Fresh embryo transfer can perform just as well and may help shorten the overall treatment timeline |
| Patients with OHSS risk | Frozen transfer is considered safer because it avoids implantation during an overstimulated cycle |
| Overall success comparison | Current research suggests frozen vs fresh embryo transfer outcomes depend more on patient profile than on one method being universally better |
Which Type of Embryo Transfer Is Right for You?
The right transfer type depends on how well the body is positioned for implantation in that particular cycle. The fresh vs frozen embryo transfer decision is not simple and is guided by several clinical factors:
- Some factors, such as age and the egg reserve, can affect both the timing of transfer and the treatment as a whole.
- In cases like PCOS or high ovarian response, frozen embryo transfer may a better decision.
- Results from stimulation can show doctors the condition of the uterus, so hormone levels play a big part here.
- Before genetic screening, you need to freeze the embryos first.
- Also, the lining of the uterus is a key factor in successful implantation.
FAQs
Does frozen embryo transfer have a higher success rate than fresh embryo transfer?
Frozen embryo transfer can show equal or higher success rates in many patients, especially women with PCOS or a strong ovarian response.
How long does a frozen embryo transfer cycle take?
A frozen embryo transfer cycle typically takes 4 to 8 weeks from starting medications to embryo transfer.
Is frozen embryo transfer safe for women with PCOS?
Yes, it is safe since frozen embryo transfer is usually recommended for women with polycystic ovary syndrome because it reduces the risk of developing ovarian hyperstimulation syndrome following IVF.
Can frozen embryos be stored for years and still work?
Yes, embryos can be frozen and stored for several years because of modern technologies, which do not affect the survival rate of those embryos.
Related Fertility Blogs