Self-cycleTM IVF
Self-cycleTM IVF

-
-
-
 Infertility Counselling
Infertility Counselling
-
 Female Infertility Treatment
Female Infertility Treatment
-
 Andrology Treatment
Andrology Treatment
-
 Fertility Enhancing Surgeries - Female
Fertility Enhancing Surgeries - Female
-
 Fertility Enhancing Surgeries - Male
Fertility Enhancing Surgeries - Male
-
 Endoscopy Treatment
Endoscopy Treatment
-
 IUI Treatment
IUI Treatment
-
 IVF Treatment
IVF Treatment
-
 ICSI Treatment
ICSI Treatment
-
 Advance IVF Solutions
Advance IVF Solutions
-
 Embryology
Embryology
-
 Vitrification Egg, Embryo, Sperm Freezing
Vitrification Egg, Embryo, Sperm Freezing
-
 Preimplantation Genetic Testing (PGT)
Preimplantation Genetic Testing (PGT)
-
 Donation Program Embryo / Egg / Sperm
Donation Program Embryo / Egg / Sperm
-
 Self-cycleTM IVF
Self-cycleTM IVF
-
-
-
-
-
Luteal Phase Defect: The Hidden Cause of Repeated Implantation Failure and Miscarriage

Most women tracking their cycles, monitoring ovulation, and doing everything right are often surprised to learn that a small hormonal shift in the second half of their cycle could be quietly affecting conception.
A luteal phase defect rarely shows up on routine tests, yet it plays a direct role in whether an embryo successfully implants and a pregnancy holds. For women with recurrent losses or failed IVF cycles, this is often where the answers lie.
What Is Luteal Phase Defect
The luteal phase begins after ovulation and lasts until the next menstrual period.
LPD occurs when the corpus luteum does not produce enough progesterone. As a result, the endometrium does not develop adequately, making it difficult for an embryo to implant and grow.
A healthy luteal phase typically lasts 12 to 14 days. If it is 10 days or shorter, it is considered clinically significant and requires further evaluation.
_0.webp)
What Causes Luteal Phase Defect
LPD is usually linked to disruptions in hormonal signaling or ovulation quality.
- Low Progesterone Production: The corpus luteum produces insufficient progesterone, directly reducing the endometrium's ability to support implantation
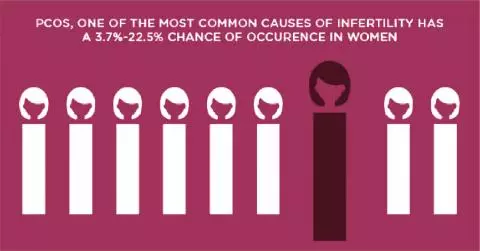
- PCOS: Irregular ovulation disrupts corpus luteum formation, making PCOS a leading contributor to LPD in Indian women
- Thyroid Disorders and Hyperprolactinemia: Both conditions interfere with the hormonal signals needed for adequate progesterone production
- Excessive Exercise or Sudden Weight Loss: Physical stress suppresses ovarian function and weakens corpus luteum development
- Stress-Induced Hormonal Disruption: Elevated cortisol disrupts the hypothalamic pituitary ovarian axis, reducing progesterone output
- Age-Related Decline: Corpus luteum function gradually weakens in women over 35, shortening the luteal phase
Signs and Symptoms of Luteal Phase Defect
LPD is frequently asymptomatic, and many women only discover it after multiple failed IVF cycles or recurrent early pregnancy loss.
When symptoms are present, they may include:
- Light spotting before periods
- Short menstrual cycles (under 21 days)
- Difficulty conceiving despite regular attempts
- Recurrent early miscarriages
- Delayed or weak rise in basal body temperature after ovulation
For women experiencing recurrent early losses, an evaluation at a recurrent pregnancy loss clinic can help determine whether LPD is a contributing factor. In some cases, what appears to be a late period may actually be a very early pregnancy loss.
How Is Luteal Phase Defect Diagnosed
A structured hormonal and imaging workup is required to confirm a luteal phase defect.
- Serum Progesterone Test: A blood test taken 7 days after ovulation to assess corpus luteum output
- Transvaginal Ultrasound: Measures endometrial thickness as a direct indicator of progesterone effect
- BBT Charting: Basal body temperature tracking to evaluate luteal phase length and quality
- Hormone Panel: FSH, LH, and estrogen levels assessed together to provide a complete reproductive hormonal picture
Luteal Phase Defect Treatment: What Are the Options
The type of treatment of LPD is determined depending on hormonal imbalance and the reproductive goals of the individual. The objective of the treatment is the promotion of higher progesterone levels, improvement of ovulation, and preparation of the endometrium for the implantation of an embryo.
- Supplementation with progesterone: Additional progesterone is administered to facilitate proper development of the endometrium to ensure that the embryo is able to implant and remain
- Human chorionic gonadotropin (hCG): It is administered to promote functioning of the corpus luteum, thus ensuring the production of progesterone
- Clomiphene citrate: It enhances quality of the egg cell produced by ovaries to increase hormone level after ovulation
- Lifestyle changes: Stress management, maintenance of appropriate body weight, and avoidance of excessive physical activity may normalize hormones
FAQs
Can you get pregnant with luteal phase defect?
Yes. With appropriate progesterone supplementation or treatment of the underlying cause, many women with LPD conceive successfully, both naturally and through assisted reproduction.
How does luteal phase defect cause miscarriage?
Insufficient progesterone prevents the endometrium from adequately supporting an implanted embryo, often resulting in very early pregnancy loss before or shortly after a missed period.
Is luteal phase defect the same as low progesterone?
Not exactly. Low progesterone is the primary indicator of LPD, but the condition also involves a shortened luteal phase and reduced endometrial receptivity, making it a broader hormonal and structural concern.
Does luteal phase defect affect IVF success rates?
Yes. An unmanaged luteal phase defect can reduce implantation rates even with good quality embryos. Luteal phase support is therefore a non-negotiable component of all IVF protocols.