 Infertility Counselling
Infertility Counselling Female Infertility Treatment
Female Infertility Treatment Andrology Treatment
Andrology Treatment Fertility Enhancing Surgeries - Female
Fertility Enhancing Surgeries - Female Fertility Enhancing Surgeries - Male
Fertility Enhancing Surgeries - Male Endoscopy Treatment
Endoscopy Treatment IUI Treatment
IUI Treatment IVF Treatment
IVF Treatment ICSI Treatment
ICSI Treatment Advanced IVF Solutions
Advanced IVF Solutions Embryology
Embryology Vitrification Egg, Embryo, Sperm Freezing
Vitrification Egg, Embryo, Sperm Freezing Preimplantation Genetic Testing (PGT)
Preimplantation Genetic Testing (PGT) Donation Program Embryo / Egg / Sperm
Donation Program Embryo / Egg / Sperm Self-cycleTM IVF
Self-cycleTM IVF
 Self-cycleTM IVF
Self-cycleTM IVFDr. Suparna Bhattacharya helps Patient with Adenomyosis, Endometriosis, Poor Ovarian Reserve become a Parent

Assisted Reproductive Treatment at Nova IVF Fertility, Kolkata helps Patient with Adenomyosis, Endometriosis & Poor Ovarian Reserve become a Parent
Mrs NC 34 years, married for eight years, visited our Nova IVF Fertility centre at Uttam Kumar Sarani, Kolkata for a consultation with our Infertility Specialist Dr Suparna Bhattacharya, MBBS, DGO.
Upon collecting patient history, we found out that this was a case of secondary infertility, indicating that the patient had at least once become pregnant. She had a previous biochemical pregnancy with self IVF and a failed IVF cycle with ovum donation in another centre.
Dr Suparna is a renowned and highly experienced Fertility Specialist in Kolkata. Since no treatments had yielded required outcomes, Mrs NC had come to our Kolkata centre, with high hopes to finally have a child.
Biochemical Pregnancy
When a patient has a positive Urine of Serum HCG pregnancy test, but there is no identifiable pregnancy on ultrasound examination, this phenomenon is called a Biochemical Pregnancy. A biochemical pregnancy thus is a miscarriage before the fifth week of pregnancy. The embryo implants in the uterus, but it never takes hold, and this loss happens so early that many may not even realize that there was a pregnancy. The cause of Biochemical Pregnancy is Genetic chromosomal abnormalities of the embryo, which prevent implantation and halt embryonic development. A biochemical pregnancy also indicates that the woman’s partner’s sperm can fertilize the egg and her uterus can allow for embryo implantation.
Patient’s detailed history and medical background
A series of pre-pregnancy tests were conducted, and detailed medical history was collected. Mrs NC had a normal BMI and had undergone a previous Laparoscopy to remove bilateral chocolate cysts. She had also undergone adhesiolysis to cure her of adhesions.
Her vitals were stable, and her abdominal examination was soft and non-tender. On P/S examination – a hypertrophied cervix with severe erosion was noticed. She also gave a history of spotting and severe white discharge post-transfer in previous cycles.
Her first USG showed an adenomyotic uterus with recurrent bilateral endometrioma and 4-5 antral follicle count. Her AMH level was 0.32 ng/ml, and husband’s semen analysis was normal.
Bilateral Endometrioma and Chocolate Cyst:
If the endometrial tissue which normally is only within the uterus, spreads to the ovaries, a cyst or lump is formed near the ovaries. Endometriomas are cysts filled with blood from ectopic endometrium and are also called an endometrial or a chocolate cyst. It is the most common form of endometriosis. Endometrioma is found in 17 – 44% of patients with endometriosis.
This cyst may be unilateral or present only on one of the ovaries, or present on both the ovaries, thus called a bilateral cyst.
While they are often small (less than 2 inches), these cysts can grow as big as 8 inches across. Ovarian cysts may be detected on transvaginal ultrasonography. Most of these are functional and therefore self-resolving in 6-8 weeks, symptom-less and benign. However, if they are large or if they do not self-resolve, they can cause considerable discomfort. Ovarian endometriomas may not impair spontaneous ovulation, and the impact of surgical excision of ovarian endometriomas on fertility needs to be further investigated .
Adhesiolysis: Patients who have undergone abdominal surgery may have bands of scar-like tissue that form between two surfaces inside the body, causing them to stick together. If these adhesions are causing problems, a minimally invasive laparoscopic procedure called adhesiolysis can help remove the scar tissue. The surgeon makes a small incision in the abdomen and uses a laparoscope to locate the adhesion. Abdominal surgery is the most frequent cause of abdominal adhesions, and everyone who undergoes abdominal surgery may develop adhesions. The risk is greater after operations on the lower abdomen and pelvis, including bowel and gynaecological surgeries.
Hypertrophied Cervix: Elongation of the cervix, this may typically happen due to recurrent infections or due to prolapse, i.e. slipping of the organ from its original position.
Erosion of Cervix: If there are recurrent infections at the mouth of the cervix, these cause erosion of tissues and if the infection is not treated and cured, this may sometime lead to much discomfort as well as diseases and will have an adverse impact on the ability to become pregnant as well as carry a pregnancy successfully.
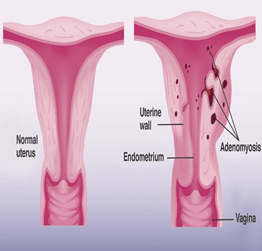
Adenomyotic Uterus: Adenomyotic Uterus is a uterus, where endometrium has grown thick and, in some places, it has made ingrowths into the uterine walls. This is call adenoma and causes a bulky uterus and massive discomfort.
Antral Follicle Count: Antral follicle count is a transvaginal ultrasound study, performed in the early phase of the menstrual cycle, in which the physician visually counts the number of egg-containing follicles that are developing on both the ovaries. The antral follicle count measures the ovarian reserve.
As a general guideline, antral follicle counts are used to determining the likelihood of success for ovarian stimulation and IVF and may also be used to guide dosing for fertility medications. Normally, 15 to 30 is considered a good number that helps the patient use her own eggs for IVF.
Treatment suggested by our IVF Fertility Specialist
Mrs NC was counselled regarding adenomyosis, and recurrent endometriomas and the treatment options suggested were an Ovum donation or a Self IVF. However, given the reduced Antral follicular count and an abnormally low AMH, using a donor was a preferred option.
Upon counselling, Mrs NC understood the complications and challenges associated with self IVF, and she willingly agreed for using donor eggs.
Successful Treatment by Nova IVF ART specialists
From her next cycle, Mrs NC was given her 1st leuprolide depot 3.75 and underwent a hysteroscopic evaluation of her uterus with TBPCR testing and a PAP smear with HPV DNA.
After all the reports came normal, a donor was recruited for her, and the embryos were frozen.
She was given two more doses of injection Leuprolide 3.75 at a monthly interval and subsequently treated for cervical erosion.
A month after her 3rd depot, her endometrium was prepared, and two good blastocysts were transferred, and injectables were used for luteal phase support avoiding the vaginal medicines.
Her HCG 10 days after the transfer was 590Miu/ml. The patient had an uneventful pregnancy and delivered a 3.01kg baby boy by LUCS, or a lower uterine segment caesarean section.
Understanding a few medical terms
- Treatment using leuprolide – Leuprolide injection is used to treat disorders of the uterus (e.g., endometriosis, fibroids) in women. It helps to reduce symptoms such as pelvic pain, painful/heavy menstrual periods, and abdominal bloating. It also shrinks the abnormal uterine tissue that causes these symptoms.
- Hysteroscopic evaluation of uterus – Hysteroscope is an instrument that is inserted intravaginally into the uterus to closely examine the uterus conditions.
- TBPCR testing – The TB-PCR test helps diagnose and confirm infection of Tuberculosis. The same had to be ruled out before starting the fertility treatment.
- Pap smear with HPV DNA – The HPV DNA test is used to check for HPV infection around the genitals in women. Some types of HPV can cause cervical cancer and other cancers; hence the same must be checked and treated adequately before the fertility treatments are started.
IVF Treatment Outcome
Nova IVF Fertility Specialists successfully treated the patient suffering from adenomyosis, endometriosis, poor ovarian reserve, and despite all her challenges, helped her become the proud mother of her baby.
The patient had severe adenomyosis with grade 4 endometriosis. She also had a very poor ovarian reserve. However, her husband’s sperm report showed normal sperm.
Despite failed previous own as well as donor cycle, and despite having a complicated medical background, the patient was able to become pregnant and had an uneventful pregnancy and delivered a 3.01 kg baby boy. This was only possible with the expert guidance of our Dr Suparna, who is a top fertility specialist in Kolkata.














Add new comment