Self-cycleTM IVF
Self-cycleTM IVF

-
-
-
 Infertility Counselling
Infertility Counselling
-
 Female Infertility Treatment
Female Infertility Treatment
-
 Andrology Treatment
Andrology Treatment
-
 Fertility Enhancing Surgeries - Female
Fertility Enhancing Surgeries - Female
-
 Fertility Enhancing Surgeries - Male
Fertility Enhancing Surgeries - Male
-
 Endoscopy Treatment
Endoscopy Treatment
-
 IUI Treatment
IUI Treatment
-
 IVF Treatment
IVF Treatment
-
 ICSI Treatment
ICSI Treatment
-
 Advance IVF Solutions
Advance IVF Solutions
-
 Embryology
Embryology
-
 Vitrification Egg, Embryo, Sperm Freezing
Vitrification Egg, Embryo, Sperm Freezing
-
 Preimplantation Genetic Testing (PGT)
Preimplantation Genetic Testing (PGT)
-
 Donation Program Embryo / Egg / Sperm
Donation Program Embryo / Egg / Sperm
-
 Self-cycleTM IVF
Self-cycleTM IVF
-
-
-
-
-
IVF Failed? Here Are the Real Reasons It Happens and What to Do Next in India

A failed IVF cycle can be upsetting, especially after all the time, effort, and hope that have gone into the treatment. However, one unsuccessful attempt does not mean IVF will never work.
Every IVF cycle provides useful information. The results can help doctors identify possible reasons why the treatment was unsuccessful and make changes for the next IVF attempt. In many cases, these changes can improve the chances of a successful pregnancy in the future.
Understanding Why IVF Fails Is the First Step Toward a Better Outcome
Many couples complete a failed cycle without receiving a clear explanation of what went wrong. They are advised to rest and try again, often without any changes to the approach.
However, a failed IVF cycle gives valuable diagnostic information that, when reviewed properly, directly shapes how the next attempt is planned.
There are many common reasons why IVF fails, and identifying which one applies to your specific cycle is what separates a repeat attempt from a meaningfully improved one. The sooner that cause is identified, the sooner the right steps can be taken.

The Most Common Reasons IVF Fails
IVF can break down at different stages and for different reasons. Understanding where your cycle failed can make the next attempt more targeted and effective.
Egg Quality and Maternal Age
Egg quality is the most frequently identified cause of IVF failure. After 35, eggs are more likely to carry chromosomal abnormalities. Even a visually normal embryo can be genetically abnormal, making implantation difficult.
Embryo Implantation Failure
The reason for embryo implantation failure is not always a single factor. A thin endometrial lining, uterine polyps or fibroids, a shifted implantation window, and poor endometrial receptivity are all established causes. Each one has a specific diagnostic test and a targeted intervention, which is why a proper cycle review is important before attempting again.
Sperm DNA Fragmentation
A standard semen analysis does not assess DNA integrity. High sperm DNA fragmentation can cause poor embryo development and increased miscarriage risk even when ICSI is used.
Many couples are unaware that sperm DNA damage is among the real reasons for failed implantation, particularly when repeated embryo arrest or poor blastocyst development has occurred.
Uterine and Hormonal Factors
Sometimes the uterus itself has structural issues, such as a septum, adhesions, or fibroids, that physically block implantation.
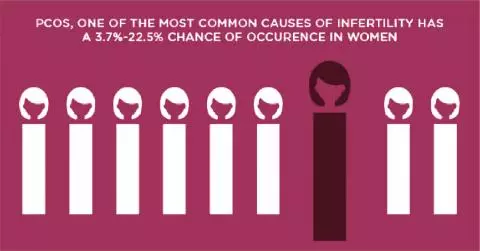
Hormonal conditions such as thyroid problems, high prolactin, or PCOS can also quietly affect how the body responds to stimulation and prepares the lining. Once these factors are identified, doctors can make changes in the plan to achieve better results in the next cycle.
What to Do After a Failed IVF Cycle
A failed cycle does not mean starting over blindly. It means you now have clinical data that can make the next attempt more precise. For couples facing IVF failure, the further steps depend on understanding the underlying reason why the current cycle was unsuccessful.
Request a Detailed Cycle Review
Before planning another cycle, ask your fertility specialist for a structured review of what might have gone wrong. This should ideally cover stimulation response, fertilisation rate, embryo grading, and transfer conditions. The goal is to identify precisely where the cycle failed, because the corrective pathway depends on that.
Consider These Four Diagnostic Tests
The right investigations after a failed cycle replace guesswork with clinical evidence. Depending on what went wrong that led to the failure of IVF, your specialist may recommend one or more of the following:
- ERA: Identifies whether your uterine lining is receptive at the time of transfer. Approximately one in three women has a displaced implantation window, meaning standard transfer timing does not match their biology. This is a common and often overlooked reason for failed implantation.
- PGT-A: Screens embryos for chromosomal abnormalities before transfer, ensuring only the healthiest embryos are selected. This directly addresses egg quality as a reason for embryo implantation failure.
- Sperm DNA Fragmentation Index: Checks for DNA damage in sperm that a routine semen test misses, relevant when embryos repeatedly develop poorly or early pregnancy loss has occurred.
- Immunological Testing: Identifies whether the immune system is actively working against implantation rather than supporting it, a cause that remains undetected without specific investigation.
A Failed Cycle Is Information, Not a Verdict
Most couples who achieve a successful pregnancy through IVF do not do so on the first cycle. What changes between attempts is the quality of information available to the clinical team. A failed cycle, when properly reviewed, tells your doctor more than any pre-treatment test could. The protocol for your next attempt should be built on that data, not a repetition of what was already tried.
FAQs
What is the most common reason IVF fails?
Poor egg quality is the most common cause. As women get older, eggs are more likely to have chromosomal problems that stop implantation from happening.
Can I try IVF again after a failed cycle?
Yes, and many couples go on to succeed in later cycles. Reviewing what went wrong and adjusting the treatment plan before the next attempt matters greatly.
Why does implantation fail even with good embryos?
Even with healthy-looking embryos, internal chromosomal defects can go unnoticed. The state and the time at which the uterine lining is will determine the success of the implantation.
What tests should I have after a failed IVF cycle?
ERA, PGT-A, sperm DNA fragmentation test, and immune tests are some of the commonly conducted tests. It is recommended to check with your fertility specialist before opting for these tests.
Related Fertility Blogs